Partners from Strategic Interests attended the annual Strategic Health Information Exchange Collaboration (SHIEC) conference in the Washington, DC area this month. This meeting brings together over 70 Health Information Exchanges (HIEs) and other interested organizations from across the country. We were able to participate in discussions, offer advice, and make some terrific connections with other interoperability experts.
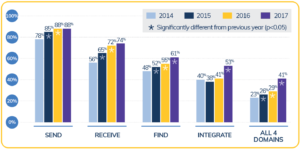
It’s been said that in healthcare, we make monumental changes at a glacial pace. According to an ONC report released this week, acute care hospitals have once again made an increase in their interoperability status versus last year. This nets out to a 2% increase in the number of hospitals that can receive patient summary of care records from other institutions, an increase of 6% for finding such records outside their health system and a whopping 12% increase in those who can integrate outside patient records into their own EHR. All told, however, only 41% of US non-federal acute care hospitals can send, receive, locate and integrate outside information – a number far too low to rush to high fives all around.
While the improvements are notable, there is still much work to do. Far too many hospitals have anemic data exchange policies and capabilities and nearly half have their EHR silo unable to show a complete patient record that includes outside care data. While we wish patients would remain within a single health system, geography, capabilities, and even travel schedules means this is often not the case.
Are you part of a hospital or health system who wants to improve your interoperability capabilities? Let Strategic Interests know. We would love to help design a suite of programs to help you achieve all the benefits an interoperable system provides.
[Strategic Interests consultant Dr. Joseph DiPoala was recently interviewed by Becker’s Hospital Review. The article is reprinted below:]
Dr. Joseph DiPoala is no stranger to electronic medical records (EMRs) and how important technology is in driving effective and insightful communication.
Co-founder of Ridgeview Internal Medicine Group, a four-physician, three-advanced provider practice in Rochester, New York, Dr. DiPoala also knows what a hassle it is to wrangle patient data from siloed sources. Not only does it take time away from patient interactions, but also increases the risk that critical data could be missed, potentially leading to less-effective treatment.
For the past 17 years, Ridgeview has thrived as a private practice. However, remaining independent comes with its challenges: Ridgeview needed to leverage interoperable technologies able to effectively communicate with other systems and share patient information.
Today, Ridgeview is empowered to connect across disparate systems, leveraging athenahealth’s Patient Record Sharing service to communicate with local large systems via CommonWell and Carequality and exchange medical information instantly. This ensures physicians have the appropriate information at the point of care and that this information follows the patient, no matter the care site. Below, he outlines how the new capability has helped fill patient information gaps during day-to-day interactions.
Q: Historically, what has been Ridgeview’s experience with sharing information with outside organizations?
A: We have had the good fortune of having an extremely well-established health information exchange (HIE) in our community with a high participation rate—but there are definitely gaps in terms of the documents that we can receive. For example, when patients get treatment in an outpatient setting for Rochester General, our main referring hospital, those records aren’t accessible through the HIE—this has been a pain point for the past three or four years. Prior to using a record sharing service, we also struggled to onboard new patients because we were unable view complete records that included previous medications and immunizations. We frequently received faxed documents and were unable to input the patient data directly from the continuity of care document (CCD). The process was a nightmare.
Q: As you mentioned, locating previous health data when onboarding a new patient is critical. What was your approach to gathering patient information before a visit?
A: Before having access to the full patient record, we received information through three sources:
• The paper medical history form patients complete when they come in: After check-in, my nurse or myself would have to transcribe the data from that paper document into the EHR.
• Records from previous visits: This was a huge tech hassle. Scanning Epic’s system—if we even had access—to find the right documents, print them out, and scan them into our system was inefficient and time-consuming. It then required a significant lift to search through the records by hand to try and identify the right information.
• Information-gathering when meeting patients for the first time: This involved filling in any gaps in the information obtained in the first two steps, and was extremely labor-intensive.
Q: What do you think is most valuable about increased interoperability?
A: Two things: First, sharing records eliminates much of the above difficulties, fills in gaps in medical histories and ensuring accurate diagnosis and treatment. Second, it brings in structured data through the reconciliation process. This way, when we see a new patient, we can not only view her records, but also import the problem, allergy, medication, and immunization lists. You can’t successfully accomplish that sort of reconciliation solely relying on faxes, information from our HIE, or other sources.
Q: Who are you exchanging records with most often? Who is benefitting from increased connectivity?
A: There are two major health systems in Rochester: Rochester Regional Health (of which Rochester General is a part) and University of Rochester Medical Center. Patient Record Sharing has allowed us to communicate with Rochester General seamlessly and, conveniently, University of Rochester Medical Center joined the network about a month or two ago. It’s been fantastic—there are only two big systems in town, and we can share records with both of them.
Q: How has exchanging patient records across systems and geographies helped you improve care coordination?
A: There is one area in particular where this has proven to be extremely valuable: When one of my patients visits the ED at Rochester General (our affiliated hospital) or at the University of Rochester Medical Center, the ED physician can see what I see as I’m able to share the record. There is peace of mind for the patient knowing no matter where they go or who they see, the physician will have access to their CCD created by athenahealth.
Q: How is interoperability key in helping you remain an independent practice?
A: For an independent practice, efficiency is critical—whenever you’re able to identify areas of inefficiency and take the appropriate steps to rectify, you’re in a better place. And now, with the ability to communicate with those around us, we’re in a much better place. Prior to sharing records, our process for securing the appropriate information at the point of care was timely and burdensome, taking physicians’ time away from focusing on the patients at hand. This is no longer the case: Instead of spending valuable time searching for missing documents and suffering from heightened, unnecessary workloads, our doctors can use that time to deliver quality care to patients.
The challenge of exchanging information among health care providers goes far beyond programming. Certainly, EHRs that use differing formats and structures increase the task of meaningful and necessary clinical data communication, but needs reach far beyond simply technology issues. Strategic priorities must be established and aligned in order for delivery of patient care to improve and the transition toward value based care to be accomplished effectively. The struggle to provide access to data is real and one that we talk to people about every day. Most patients, and even many doctors, assume all pertinent data is available to anyone who should be granted access. This is simply not the case in most communities.
Public health information exchanges have attacked some of the problems, providing a public utility of sorts to manage the flow of information. And private HIEs close gaps for some institutions, especially following mergers and acquisitions of practices and health systems, but integral to the process of interoperability is stakeholders achieving alignment with goals, plans and initiatives.
In order to ensure the right data is presented to the right people at the right time, and the creation of a truly integrated EHR is available, a course of action can include multiple tools, APIs, options and approaches. For some systems, a single EHR can be used including add-on modules to incorporate data. In other situations, such as when legacy data is required to be accessible from retired EHRs or when many data sources are using a variety of different systems, custom built or customizable off-the-shelf interface engines might be the best choice.
Decisions abound but one thing holds fast — tackling interoperability strategy shouldn’t be done in a vacuum. Using objective strategic advisors to collect requirements, assess cultural implications, evaluate vendor offerings and help to plan the most effective and efficient path will save costs, headaches, and, in the end, lives through the improvement in patient safety and care quality.
Chicago, August 2017 — Al Kinel discussing care transition IT strategy at Allscripts Population Health University
As part of the Allscripts Population Health University held August 8 – 10, 2017 at Chicago’s McCormick Center, Strategic Interests president, Al Kinel, led a presentation explaining the improvement of care transitions using information technology. As seasoned implementation agents for Allscripts dbMotion product, SI understands first hand how the timely exchange of pertinent information positively impacts transitions of care from clinical, technical and strategic angles.
Kinel was joined by two SI clients who discussed their experience with interoperability and transitions of care: Erik Jacob, Manager of IT Interoperability at Rochester Regional Health, discussed the projects in Rochester from the Community Diabetes Collaborative through the merger of multiple hospitals and practices. Brian Henderson, Director of Physician IT Services at Sarasota Memorial Hospital presented the project connecting ambulatory community providers to the hospital’s health information exchange, SMHxchange. Finishing the talk, Strategic Interest’s Director of Clinical Services, Brett Kinsler, DC presented the methodology used to identify gaps and prioritize data elements to be exchanged to facilitate a Medicaid DSRIP program.
Chicago, August 2017 — Erik Jacob presented Rochester Regional Health’s interoperability process
Overall, the team defined the value of Health Information Exchange (HIE) with specific use case examples and described how innovative solutions can impact organizations and practices, increase care quality, decrease duplication of services, prevent unnecessary readmissions, and enable innovative payment models while attaining strategic objectives and enhancing partnerships among hospitals, LTPACs and community providers.
We appreciate being invited by Allscripts to present a topic we are so passionate about and are grateful to our client partners from RRH and SMH for bringing real life examples and experience to the discussion.
When it comes to EHR (electronic health records) improvement projects cited among healthcare organiation executives, the plan to improve connectivity with other systems topped plans for 2017. According to Healthcare IT News’ recent survey of 96 respondents, sixty percent of those polled are planning or are already in the midst of an interoperability initiative. Most of these projects (65%) involve connecting to external databases or health information exchanges (HIE).
These executives recognize that there can be challenges to interoperability, listing the lack of industry standards, EHR vendors themselves, the “culture of hoarding,” and financial concerns.
“The Year Ahead in Health IT” survey also identified emerging technologies many organizations had plans to invest in this year. This included prescriptive analytics, artificial intelligence, genomic tools and machine learning, cognitive computing, and blockchain.
Where is your organization on the path to interoperability and leveraging technology to improve quality of care, save costs and become more efficient? A seasoned healthcare technology consulting firm can be your guide to strategy, design and implementation while helping you navigate the tricky areas of vendor management and balancing internal change management.



 When it comes to EHR (electronic health records) improvement projects cited among healthcare organiation executives, the plan to improve connectivity with other systems topped plans for 2017. According to Healthcare IT News’ recent survey of 96 respondents, sixty percent of those polled are planning or are already in the midst of an interoperability initiative. Most of these projects (65%) involve connecting to external databases or health information exchanges (HIE).
When it comes to EHR (electronic health records) improvement projects cited among healthcare organiation executives, the plan to improve connectivity with other systems topped plans for 2017. According to Healthcare IT News’ recent survey of 96 respondents, sixty percent of those polled are planning or are already in the midst of an interoperability initiative. Most of these projects (65%) involve connecting to external databases or health information exchanges (HIE).
Recent Comments